|
|||||||||||||||||||||
 |
|||||||||||||||||||||
 |
|||||||||||||||||||||
 |
|||||||||||||||||||||

















|
|
"AIDS is the number one cause of death for African Americans between the ages of 25 and 44. That is startling.... Today you're going to hear many reasons why AIDS is on the rise again. And here's a shocker. It's one of the big reasons why so many women are getting AIDS: Their husbands and boyfriends are having secret sex with other men... OK? OK? This lifestyle even has a name. It's called living on the down low. Have you heard about it? " [1] The date was April 16, 2004. The words were those of Oprah Winfrey leading off that Fridays version of her long running syndicated daily TV show. But instead of information on the promised many ways you can get AIDS, what Oprahs audience got was an hour of disinformation, stereotyping and hucksterism. They got just one way to avoid the deadly infection, from one source: secretive and predatory bisexual black men, Living on the Down Low. During that hour, Oprah and her guest, J.L. King, the author of what became, thanks to exposure on Oprah TV show and web site, a best selling book, did incalculable and lasting damage to the battle for HIV-AIDS prevention, treatment, and understanding of the epidemic in the African American community. Huckster J.L. King portrayed himself as a typical example of a down low brutha, supposedly reformed just enough to want to sell his book and services as a speaker, passing on tidbits of useful information such as where he and other down low bruthas go to meet each other:
 Among the sage bits of advice
King had for black women on the lookout for signs of down-lowness
in their sweethearts and spouses, was to watch their eyes, pay
attention to their gay friends, to follow them around.
Mr. King isnt selling public health advice hes selling public hysteria, and thanks to his exposure on the Oprah show, King now makes a good living off it.
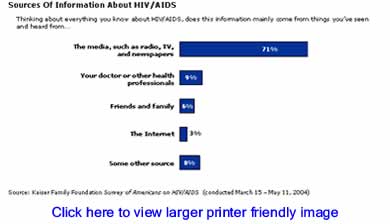
Although Oprah Winfrey is not a public health professional, what she says and what she allows to be said on her show concerning the AIDS epidemic definitely matters. According to the Black Aids Foundation, one of whose representatives did appear in the final minutes of the April 16, 2004 Oprah show, the number of print and broadcast news stories about the domestic AIDS epidemic declined by 57% between 1997 and 2002, during which time the occurrence of new HIV-AIDS cases among whites declined. Since then, the incidence of new HIV-AIDS cases has spiked in the African American community, but without an attendant increase in coverage. The Kaiser Family Foundation confirms that it is the popular media which provide the public with most of what they know about the epidemic.
Its not Oprahs fault that news we can use about the HIV-AIDS epidemic in black America is so scarce. But it is precisely the lack of information about this burgeoning public health crisis which imposes moral and ethical responsibilities on communicators and broadcasters, especially those with large audiences directly affected by the epidemic to get it right. The Oprah show and fearmongering AIDS hustler J.L. King instead got it very, very wrong. The real lowdown on the down low is that it just aint true. Most of the existing HIV-AIDS cases are not gay men, and hedonistic bisexual black men on the DL are NOT the major vector of virus transmission to black women. Is it True? Does it Matter? Oprahs declaration that secretive and predatory bisexual black men, of whom author J.L. King offered himself as a typical example, were in some large part responsible for the AIDS epidemic one of the big reasons why so many women are getting AIDS was then and remains today factually untrue. BC will not speculate on how the fraudulent nature of this claim eluded the Oprah shows producers some 17 months ago. But for a good while now, anyone with Internet access has been able to bring up the search engine www.Google.com and type in the terms HIV-AIDS + downlow (without the quotes). The topmost result is a page from the Center for Disease Control titled FAQ Men on the Down Low. It says, in part:
There it is in black and white. When you ask the Centers for Disease Control about this down low stuff the first things they tell you are that they dont know whether or not DL bruthas account for more HIV transmission to women than men who inject drugs. They dont know whether DL bruthas are more likely to be HIV infected than other men, including exclusively heterosexual men. There is no data to back up Oprahs assertion that DL behavior is one of the big reasons why so many women are getting AIDS. We at BC are not the first to note that the Oprah Winfrey show and Down-Low author J.L. King are in deep disagreement with the Center for Disease Control, and with the known facts of the AIDS epidemic. Of the eight medical doctors, public health professionals, HIV-AIDS treatment and testing providers and advocates on the case level and the policy level whom BC interviewed for this article, not one could be found to co-sign the notion that down low bruthas are chiefly responsible for the epidemic of HIV-AIDS among black women. We humbly suggest that Oprah owes her audience a sincere and profound apology for popularizing this damaging myth, and a follow-up show that features real doctors, real HIV researchers, real public health professionals who minister to the epidemic on a daily basis, along with real advocates of testing, treatment, healing and prevention. A great place to start might be someone from the Black AIDS Foundation, who only got a handful of words in edgewise in the final moments of the infamous down low show. BC Consults a Doctor/Researcher To see how easy it might be to follow our own advice, BC looked around for a real medical doctor to ask about the down low, one involved in public health issues as they relate to the black community. Dr. David Malebranche, an MPH and assistant professor of medicine at Atlantas Emory University, has been speaking, writing and conducting research on public health issues and HIV-AIDS for some time.
Its a racist slander, Dr. Malebranche told BC when we asked him what he thought of the proliferation of media stories about the DL. At the 2004 International AIDS Conference he had this to say about the Oprah show and the DL hype machine:
Still, the hype goes on. J. L. King and others who counsel scapegoating, suspicion, misdirection and the bulk purchase of their books continue to be celebrated in the media and prosper on the lecture circuit. BC asked Dr. Malebranche why TV and the media publicize lurid and bogus allegations while stories based the findings of real researchers and treatment professionals are so rare. His answer was illuminating. Because those findings dont demonize black men, answered the good doctor.
We add to that trenchant observation this selection from Emory Universitys Emory Report, summarizing a recent study published by Dr. Malebranche and co-author Greg Millet of the Centers for Disease Control:
Secretive sexual behavior has been around since the dawn of time, said Dr. Malebranche to BC. Why is it that now we need a new name for this behavior, aside from our need to blame and demonize black men, and distract our attention from whats really going on? Aside from injected drug use, most of it [AIDS] comes from one place unprotected sex. And most of the sex that most of us are having and continue to have with partners of the same or either sex continues to be unprotected. Its foolish, and in the context of an epidemic its dangerous to imagine that so-called down low brothers have a corner on the market for risky behavior or unprotected sex. They dont. We all have a hand in this. BC thinks Dr. Malebranche is onto something here. The myth of the downlow fails to accurately explain where the virus comes from or equip us to protect ourselves and each other. It is both a racist and a homophobic slander. Oprahs producers must have known that however false and misleading it might be, their down low show would attract viewers and be remembered by them, just like that low-down hustler J.L. King knew it would sell books. The market has an endless appetite for shocking tales of unique black depravity. We need look no further than last weeks reports broadcast around the world of sniper fire halting the helicopter evacuation of hospital patients in New Orleans, which the FAA now confirms never happened. BC suspects we may be seeing a new kind of defamatory offensive against African America, in which some of the worst pathologies of white America are projected by its corporate media upon us. One such canard currently in wide circulation holds that the African American community in general, and especially the black church, are, unlike their white counterparts, bastions of virulent homophobia. Certainly there is no doubt that black homophobia exists, and that many backward pastors drink and dispense from this poisoned well. Its also true that gay male musical directors in black churches are prevalent often enough to be a kind of cliché. Nobody at BC has spent much time in white Baptist churches, but we doubt they see much of that, or that gay band leaders and drum majors are a cliché in white colleges either. BC Consults an HIV-AIDS Treatment Professional
As Executive Director of the South Carolina’s HIV-AIDS Council, Dr. Bambi Gaddist has been on the front lines of HIV-AIDS treatment and advocacy a long time. She has a PhD in Public health. In our conversation with her about the “down low,” homophobia, the black church and the AIDS epidemic Dr. G addist recounted that for years there have been several standard questions she has asked every person who comes through her agency’s doors for service, and which she has also asked many hundreds of people for whom she has done workshops and presentations. Among those questions are:
Uniformly, Dr. Gaddist reports, those questioned say they were under 20, used no protection and doubt anyone could have said anything to prevent the encounter. African Americans concerned about the HIV-AIDS epidemic are not well served when we allow lurid conversations about the down low to take up all the oxygen in the room There are vast disconnects between what we as peers and parents tell each other, between what many of our churches are telling young people, and what we are actually doing, and yet another disconnect between that and what we must do to get a handle on this epidemic, says Dr. Gaddist. HIV-AIDS is not a gay disease, and down low bruthas are not lurking everywhere, but the virus could be anywhere Its the spirit of shame, fear, and judgment that continues to perpetuate the spread of the virus throughout our community and families. Dr. Gaddist added that the South is now ground zero for the black HIV-AIDS epidemic, its 36% of the US population accounting for 40% of the nations AIDS prevalence (existing cases) and 46% of AIDS incidence (new cases) in 2003. If HIV-AIDS was a gay male disease, she points out, why is it on the decline in the western and northeastern US, but on the rise in the south, including the rural South? The answer is that HIV-AIDS is increasingly a black disease, and the southern states is where half of us still are. Dr. Gaddist believes that, notable exceptions aside, there is plenty of hope and love for all Gods children, regardless of sexual orientation, within the African American church. Its leaders, she says, have a vital role to play in bringing a halt to the epidemic. Bishops, pastors, and those entrusted with the authority to guide their flocks are now, more than ever, being called to unconditional love for the least of these. The South Carolina HIV-AIDS Council exists to help them answer that call. Where America Refuses to Look For HIV: The Prison Industry An obvious, overlooked and under-researched vector of HIV-AIDS into black women and black communities is the planet’s largest prison industry, right here in the United States. The US leads the world in the numbers and the percentage of its citizens behind bars. Black America, representing just one-eighth of the nation’s population, contributes about half of the prison industry’s human raw material. Despite mountains of anecdotal evidence, little research to date has been done on the incidence and prevalence of HIV-AIDS in America’s prisons and jails, and the relationship between the epidemic on either side of the walls.
“The Time is Now: The State of AIDS in Black America”, is a compelling, authoritative and easy to read document issued by the Black AIDS Foundation in February 2005 which we highly recommend to any and everyone. It addresses the prison-HIV connection first by pointing out that the grossly disproportionate rate of black incarceration exists alongside the soaring rate of HIV-AIDS infection:
But that’s exactly what we do when we concentrate on myths and distractions like the hunt for those ubiquitous and invisible “DL bruthas.” Just as much of black America’s leadership is content to ignore the fact of our nation’s disastrous public policy of mass incarceration of black youth, we have so far turned a blind eye to the growing the threat to public health posed by the epidemic in America’s prisons, where again, we are the majority. Prison industry officials, for their part, are doubtless fat and happy to be so ignored. Many states and large counties, have privatized inmate health services too, creating an additional large disincentive to prevention, testing or aggressively treating HIV and hep C positive prisoners. BC believes that South Carolina is one of only two states that tests inmates on entry for HIV, offering them counseling and in some cases sending them to separate facilities. The Good News TV shows like Oprah’s try to end on a positive note --- a ray of light, a success story, a glimmer of hope. BC didn’t have to look far for this either.
Last month in Illinois, where African Americans make up 15% of the state’s population, are 51% of the diagnosed AIDS cases, and 65% of the prison census, activists successfully enacted groundbreaking legislation that enables Chicago State University to conduct the nation’s first comprehensive study of the connection between the HIV-AIDS epidemics in prison and in the state’s African American communities. We talked to Chicago’s Lloyd Kelly of the Let’s Talk, Let’s Test Foundation, one of the principal advocates behind this initiative.
The Illinois legislation does not provide for mandatory testing of prisoners. “That would be a bad idea,” said Kelly. “Inmates have rights too…. Who are we to tell people they have to be tested, given the consequences of coming up positive?” Brother Kelly’s point, and we think he is right, is that potential employers, landlords and other parties have been known to acquire people’s medical records through various means and discriminate against people who are HIV-positive. Ex-offenders have enough to deal with already without compulsory HIV testing. Just as placing exclusive blame on bisexual black men for the HIV epidemic is unproductive, scapegoating prisoners is wrong too. Among the provisions of Illinois House Bill 2578, according to an August 19 Chicago Tribune article:
Community groups, Kelly told BC, will be able to walk up to people in line getting drivers licenses or applying for unemployment benefits, and administer an HIV test with results in 20 minutes. Additionally, there is to be a permanent panel including two ex-offender reps who will review implementation of the act. A provision for the distribution of condoms was struck from the law late in the process to ensure its passage. Called the HIV-AIDS Response Act, it awaits funding in the next session of the Illinois legislature.
There is no doubt that the Oprah show which featured low down J.L. King and helped legitimize his ghetto-centric and homophobic boogeyman theories about the spread of HIV set back the cause of addressing the epidemic which is ravaging black America. The DL boogeyman does not begin to explain the facts of the HIV epidemic, in which substantial proportions of infections occur daily from injected drug use, from sexual contact with an injected drug user or someone else who has been with such a user. It doesn’t take into account the prison factor, and it allows us to forget that many heterosexual men as well as women have multiple undisclosed partners and are unprotected with many, most, or all of them. Besides allowing us to ignore or evade responsibility for our individual and collective sexual behavior, discussion and media hype over the DL hype diverts attention from commonsensical public policy measures like those recommended by the Black AIDS Institute’s “The Time is Now,” which call calls for engaging HIV “not only as an individual health concern, but also as a political and social struggle.” Those recommendations, on pages 7 and 8 of the report are
The “DL brutha” is a boogeyman, and boogeymen are for children. When we become adults, we cast aside childish things. It’s time to send the DL boogeyman back to wherever he came from. Oprah helped unleash that boogeyman. Will she help bury him? Bruce Dixon can be contacted at [email protected] [1] Transcript of the Oprah Winfrey show, A Secret Sex World: Living on the Down Low, Executive Producer Ellen Rakieten, April 16, 2004, page 2. Downloaded transcripts from the Oprah Winfrey show are only $6. [2] Ibid, P, 11 |
Your comments are always welcome. Visit the Contact Us page to send e-Mail or Feedback or Click here to send e-Mail to [email protected] e-Mail re-print notice
If you send us an e-Mail message we may publish all or part of it, unless you tell us it is not for publication. You may also request that we withhold your name. Thank you very much for your readership. |

| September 8 2005 Issue 149 |
|||||||||
|
|||||||||
|
|
|||||||||
| Printer Friendly Version | |||||||||
 |
|||||||||
 |
|||||||||
 |
|||||||||
 |
|||||||||
 |
|||||||||
| |
|||||||||
| |
|||||||||